- Introduction to Neonatal Resuscitation
- The Fetal-to-Neonatal Transition
Introduction to Neonatal Resuscitation
The goal of neonatal resuscitation is straightforward: support the newborn through the critical transition from fetal to independent life, and intervene promptly when that transition is impaired. While the majority of newborns make this transition without assistance, a meaningful proportion require help, and every birth carries some probability of requiring resuscitation, regardless of how uncomplicated the pregnancy appeared.
The clinical principles throughout this course align with ILCOR 2025 guidelines, whether you're preparing for initial certification or renewing.
Who Needs Resuscitation?
Approximately 10% of newborns require some form of stimulation or assistance to establish effective breathing at birth. Of those, roughly 1% require advanced resuscitation interventions: positive-pressure ventilation, chest compressions, medications, or advanced airway management. In absolute numbers, this translates to tens of thousands of newborns per year requiring resuscitation across delivery rooms, birthing centers, and emergency settings.
Half of all newborns who need resuscitation arrive with no prenatal warning. Preparation cannot be reserved for flagged deliveries. Every birth team must be ready.
The Neonatal Resuscitation Framework
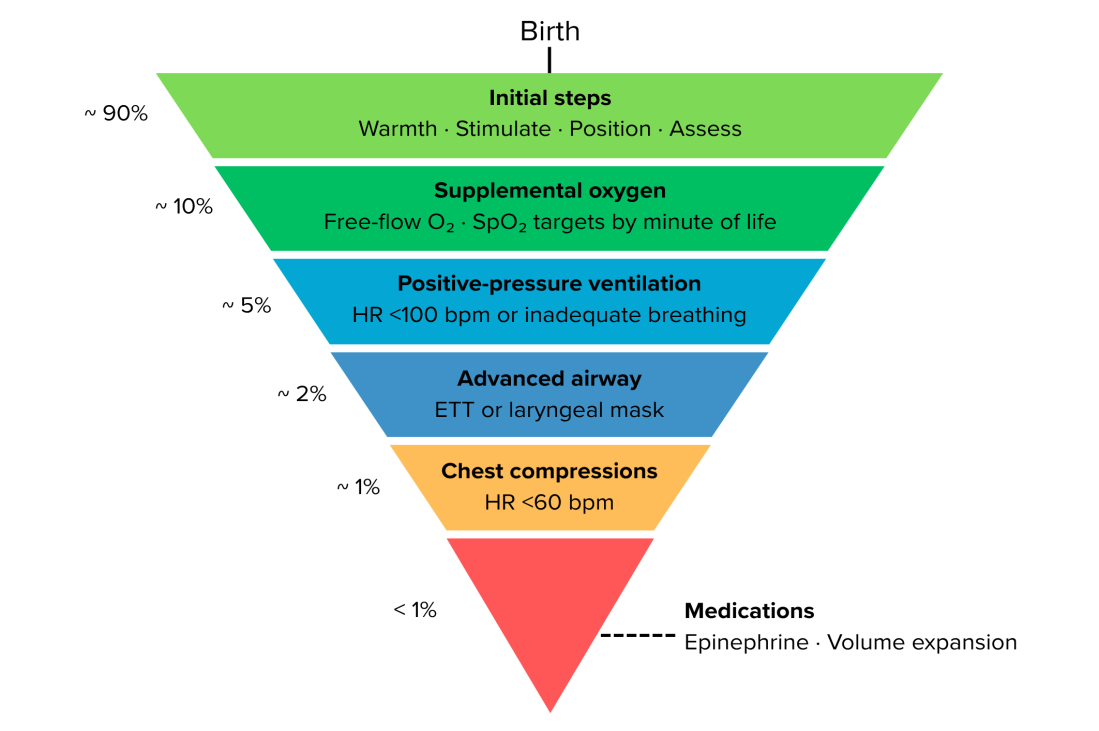
All neonatal resuscitation decisions follow a structured framework represented as an inverted pyramid (Figure 1). The widest band (applied to virtually every newborn) represents the initial steps. As the pyramid narrows, each successive level of intervention is required by fewer infants. Progression from one level to the next is always contingent on the infant's response to the current intervention remaining suboptimal within a defined timeframe.
The 60-second Golden Minute
The Golden Minute is the period from birth to the initiation of positive-pressure ventilation, if required. A newborn in secondary apnea cannot recover without ventilatory support, and delay in initiating PPV increases the risk of hypoxic injury. The initial steps (warm, stimulate, position, and assess) must be completed efficiently enough that PPV can begin within 60 seconds of birth if the infant's response is inadequate.
Team-based care
Before every delivery, roles should be assigned: team leader, airway provider, compression provider, medication administrator, and documentation recorder. Anticipation and role clarity at the outset are as important as technical proficiency during the event.
All providers participating in neonatal resuscitation should be proficient in basic newborn assessment and initial steps. This course builds from that foundation toward advanced resuscitation decision-making.
Medically reviewed by: Kim Murray, RN, MS., Medical Educator