- Initiating Positive-Pressure Ventilation
- Assessing PPV Effectiveness and Corrective Steps
Assessing PPV Effectiveness and Corrective Steps
Ineffective PPV, defined as PPV that is not producing adequate lung inflation, will not improve the infant's condition and delays escalation. Every provider must be able to assess PPV effectiveness in real time and apply corrective steps when the response is inadequate.
Assessing PPV effectiveness
PPV effectiveness is assessed by three concurrent indicators:
- Chest rise: visible, bilateral chest rise with each breath is the primary indicator of adequate lung inflation. Rise should be gentle, not exaggerated. Excessive rise indicates over-inflation.
- Breath sounds: bilateral breath sounds confirmed by auscultation support adequate ventilation, though they are secondary to chest rise assessment.
- Heart rate: a rising or sustained heart rate above 100 bpm is the definitive indicator that PPV is effective. Heart rate is the most important clinical response to monitor during PPV.
If chest rise is absent and heart rate is not improving within 15-30 seconds of starting PPV, corrective steps must begin immediately. It is important that you do not continue ineffective PPV.
Corrective ventilation steps (MR SOPA)
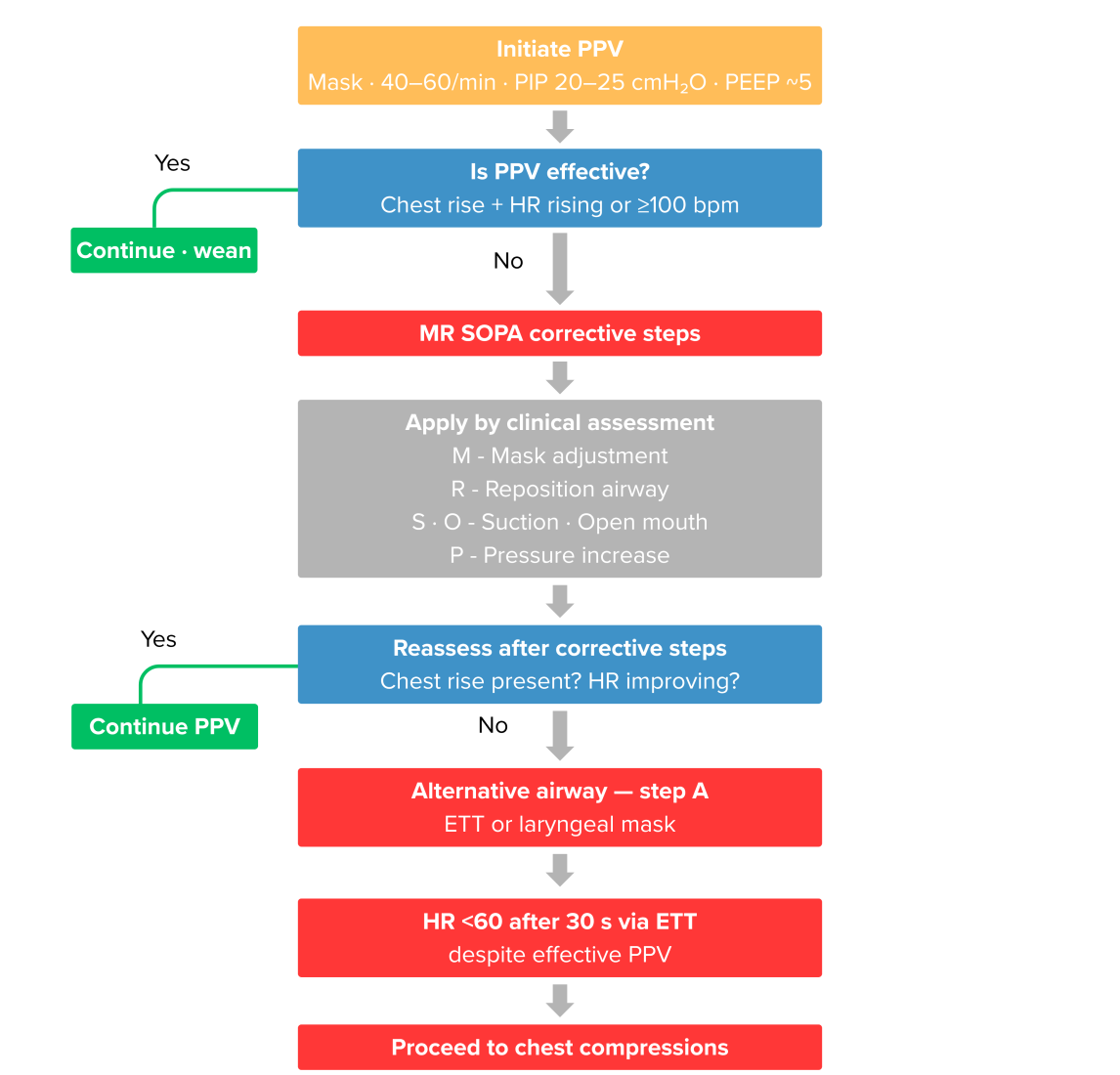
MR SOPA is an acronym used to remember the corrective ventilation steps: Mask adjustment, Reposition airway, Suction, Open mouth, Pressure increase, and Alternative airway. Current guidelines revised the approach to these steps.
Rather than following a fixed sequence, steps are now initiated based on clinical assessment of the most likely cause of PPV failure. If no chest movement and no heart rate improvement are present within 15-30 seconds, begin corrective steps prioritised by what the clinical picture suggests (Table 9):
Step | Action | Most likely cause addressed |
|---|---|---|
| M - Mask adjustment | Reposition and reseal the mask; recheck E-C hold | Mask leak |
| R - Reposition airway | Return head to neutral sniffing position; avoid flexion or extension | Airway obstruction from positioning |
| S - Suction | Suction mouth then nose with bulb syringe or catheter | Secretions obstructing airway |
| O - Open mouth | Open infant's mouth slightly; consider oral airway adjunct | Tongue or soft tissue obstruction |
| P - Pressure increase | Increase PIP by 5–10 cmH₂O increments up to 30-40 cmH₂O | Insufficient inflation pressure |
| A - Alternative airway | Proceed to ETT or laryngeal mask airway | Persistent failure despite M-R-S-O-P |
Mask adjustment and airway repositioning address the two most common causes of PPV failure and should be tried first. Suction and open mouth follow if those steps are insufficient. Pressure increase is applied when the airway is confirmed patent but chest rise is still absent. Alternative airway is the step of last resort.
Pulse oximetry placement
A pulse oximeter probe should be placed on the right hand or wrist (the preductal position) at the start of PPV. This location reflects cerebral oxygen delivery, which is what matters during active resuscitation. Postductal readings from the left hand or lower limbs may be significantly lower and should not be used to guide oxygen titration.
When to escalate beyond PPV
PPV should continue until one of the following occurs:
- Heart rate rises above 100 bpm with improving respiratory effort: begin weaning PPV, transition to observation
- Heart rate remains below 60 bpm despite 30 seconds of effective PPV via ETT: initiate chest compressions
If the heart rate fails to rise above 60 bpm despite corrective steps and adequate PPV, escalation to chest compressions is required. The full PPV decision pathway from initiation through escalation is summarised in Figure 3.
Effective PPV is confirmed by a rising heart rate (not by chest rise alone). A newborn with improving chest rise but persistent bradycardia is not responding adequately and requires reassessment of ventilation quality and escalation threshold.
Medically reviewed by: Kim Murray, RN, MS., Medical Educator